No conflicts of interest
Synopsis
Cellulite is universal mainly in females but also males can be stricken. It was thought to be related only to female secondary sex characteristic but lately shown to be a multilevel condition where structural bands, differences in subcutaneous anatomy, fat accumulation, local inflammation, superficial fascia and skin laxity can play a role. The term cellulite was first reported in the French literature 150 years ago and during 1600s it was even portrayed by artists in their paintings. In this chapter we will connect the dots to improve the understanding of the pathophysiology, causes and treatments available for Cellulite.
What is Cellulite?
History
The medical terms are liposclerosis or edematofibrosclerosis and popularly known as bumpy or unevenness texture of the skin, “cottage cheese” or “orange peel”. The classical sign of cellulite is the dimpling and commonly appear on the buttocks, thighs, or hips, but can also be seen in arms and abdomen. It mostly affects women but approximately 2% of men are affected as well. Cellulite is a characterized by changes in the cutaneous surface (depressions or subcutaneous fat pseudoherniation, which is clinically visualized as bulging). According to Orentreich and Hexsel, these findings are due to the anatomic characteristics of the lamellar layer of the female subcutaneous tissue, which, unlike the male, is composed of large, square-shaped adipose tissue lobes separated by connective septa. This septaes would thicken and shorten due to trauma in the area or inflammation resulting in skin traction, which is clinically are represented by dimples. Due to weight gain and edema those fat lobes do bulge and retract the region of the septa. There are also changes in dermal layer, due to intrinsic ageing , causing thinning and loss of dermal support and leading to micro-herniation of adipose tissue which would explain partially why, even without weight change, cellulite can worsen with age.
The full pathophysiology of cellulite is still a matter of debate in the scientific community . There are three main theories about cellulite’s etiology:
-1) Nürnberger and Muller: is based on the different architectural structure of subcutaneous tissues in male and female. Using TC, they described the female subcutaneous and dermal compartment as constituted by collagen fibers organized in rectangular lobules surrounded by branches of collagen disposed perpendicularly to the skin surface, while male subcutaneous and dermal compartments are characterized by the deposition of collagen fibers randomly disposed in the tissue, in order to form small polygonal lobules . Nürnberger and Muller confirmed, in females, the thickening of collagen fibers that surround the lobules, affecting its protrusion, which is composed by mature adipocytes
compressed inside each lobule. This mechanism is influenced by estrogen causing the protrusion of these papillae adiposae visible only in women .
-2) Merlen and Curri: is based on the hypothesis of vascular changes. The authors described a different pattern of lymphatic drainage and blood circulation in cellulite-affected tissue that leads to the development of fibrosis.
-3) Gruber and Huber and Draelos: attributes the development of cellulite to the chronic inflammation subsequent to the estrogens’ action and to the deposition of glycosaminoglycans (GAGs) by dermal fibroblasts
All the theories above are well recognized and accepted but still do not explain fully the pathophysiology of cellulite, therefore there is still space for research in this field. An interesting question would be where really everything starts, what is the initial trigger and maybe the answer is within the embryology and stem cells different responses to stress. A new line of research on the subject is rising to investigate the MUSE cells (multi-lineage differentiating stress enduring), a subpopulation of mesenchymal stem cells with special regenerative capability that are stress-tolerant and pluripotent. Conti et al in 2020 identified MUSE cells in cellulite-affected tissue and in further studies investigated how these stem cell subpopulations play a role in the cellulite etiology. In an early phase of cellulite development these cells could have a role in the dermis adipose tissue modification. They are present close to mature unilocular adipocytes and to sweat glands and in cellulite affected tissue presented an augmented number of MUSE cells suggesting a possible role in this pathology The study suggested that during cellulite development the mesenchymal stem cells have a pivotal role for their affinity to estrogen and stress , (oxidative stress, matrix remodeling, reactive oxygen species production) recruitment, as demonstrated by proteomic analysis.
Anatomy behind it: from skin to superficial fascia
The first publications on cellulite described as main factors of the condition : accumulation of fat, local edema, inflammation and herniation of areolar fat to the dermis. It took some years to understand that the major issue was somewhat related to the fat accumulation, pressure on the septae and distribution of this septae. It was not until 2002 that image studies such as MRI in vivo were used to compare the anatomy of the subcutaneous in between gender and also women who had cellulite and the ones who had not. Querleux in 2002 showed with 3D MRI that the subcutaneous anatomy in the three groups were very different. The women with cellulite presented a much less dense number of septae layer in between dermis and superficial fascia but much thicker ones compared to women without cellulite who had much denser number of septae layer and thinner sepates, and if compared to men the last one had an even denser connection with not only vertical direction but also horizontal and parallel to the skin like a strong net. (FIGURE 1) Further on, Ducan describe the aging of the fascia layer comparing, through electron microscopy, ages 23/41 and 60 years old showing that there is an intense loss of density with the years. In 2018 the superficial fascia layer (SFS) took the podium and the understanding that the tension on this layer depends not only septae but this layer would be part of a full system called by the authors as skin envelope: superficial fascia (SF), septaes(S), superficial fat (SFL), dermis (D) and epidermis (E). The maintenance in the tension on skin envelope (SE) is queen to improve cellulite. In 2018 Casabona showed that if the skin envelope is improved, with non invasive procedures that only stimulate collagen and elastin production in SE layers, the cellulite appearance could be improved. If we look at Querleux study the images show clearly that the SF is almost not visible in women with cellulite compared to women or men without cellulite reinforcing the theory that the cause is much more related to the fascias system than we predicted before. Also in the beginning it was believed that fat accumulation was one major pilar among causes of Cellulite, followed by inflammation and alterations in structure of the dermal-epidermal component, but in fact it does not explain all the cases. How to explain than that women after 35 years even without any BMI or weight changes or aged dermis start having cellulite? It was in 2018 that Casabona et al published a study where 150 people divided by gender, BMI and age suggested that there is a shift in fat layer. When we age, especially women, the fat from the superficial fat layer (layer that belongs to the skin envelope) shift to the deep fat layer . On top of that the gain in pressure in deep fat put pressure on the skin envelope and pull the structural bands and this could explain why women over 35 can start having cellulite. As Rudolph et all, beautifully showed in 2019, the anatomy of the skin envelope and the pressure and forces in between the superficial and deep fat layer are the major components of this universal condition. and In more detail: (FIGURE 1)

Gender influence
Callaghan et all showed through confocal microscopy in vivo that in contraction the septae behaviour in man and women is different. Confirmed later by Rudolph that published a study comparing cadaver dissections of men and women, the superficial fascia system in men have many more septae and they are perpendicular to the skin giving a bigger support against pressure, on the other hand women have a more oblique distribution of the septaes and have less number, therefore a softer and less strong force against contraction and pressure..
Pierard et all showed in autopsy samples with histology that there is a protusion of fat layer into de dermis of women with cellulite
Querlux et all used MRI to evaluate the thickness of fat layer and it showed that women with cellulite presented a thicker fat layer
BMI influence
Against past beliefs Casabona et al showed that when we gain weight we gain fat in superficial and deep fat layer which increase even more the pressure applied to the septae and the dermis.
Other Factors
Rossi and Vergnani theory defend that there is a big influence of estrogen in pathophysiology of cellulite. The enhanced estrogen liberation in women activate fibroblasts to produce more glycosaminoglycans (GAGs) which enhances the osmotic pressure leading to fluid retention and smaller lymphatic drainage explaining the edema accompanying cellulite regions. On the other hand when menopause takes place and there is less estrogen production with and increase activity of the lipoprotein lipase activity tat correleates to accumulation of abdominal fat in women and central obesity worsening, therefore, cellulite in other regions such as abdomen and arms.
Diagnosis
Clinical differences
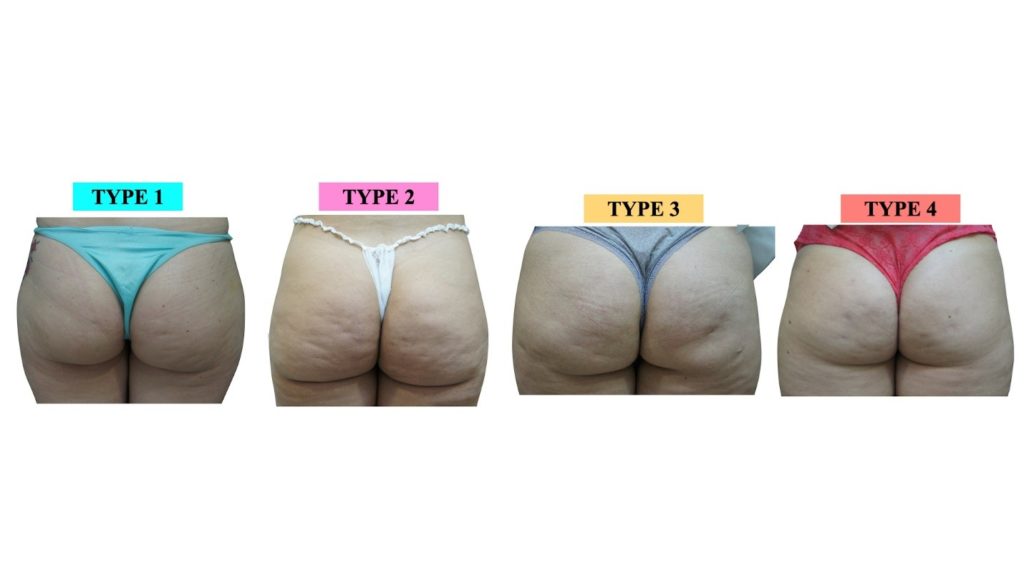
There are 4 Types of cellulite according with combination of scales( table 2, Figure 2 ): Type 1 – mainly structural just dimples no skin laxity or fascia laxity and normal BMI, Type 2 dimples with skin laxity but normal BMI or region fat volume, Type 3 dimples with skin laxity and high BMI or enhanced fat volume in the region and Type 4 dimples with no skin laxity but high BMI or enhanced volume of fat in the region. Although we have some published classification for cellulite it only take into account the appearance of dimples and peau d’orange but not really the concrete laxity factor involved in the conditions appearance. So below we will describe a way of evaluating the cases using scales both of dimples and laxity that can guide to better shape and develop a efficient plan of combinations to get the best result for the shock treatment.
TYPES OS CELLULITE
| PARAMETERS | 1 | 2 | 3 | 4 |
| DIMPLE SCALE | 0-4 | 0-4 | 0-4 | 0-4 |
| LAXITY SCALE | 0 | 0-4 | 0-4 | 0 |
| VOLUME SCALE OR ACTUAL BMI | 0 NORMAL | 0 NORMAL | 0 HIGH | 0 HIGH |
A different view on cellulite treatment
Vectors – The What
Its is well stablished in publications that we age in layers. So the speed of ageing can be different and also intensity of ageing of each layer but what does it means clinically? What is the role of the ageing of the superficial fascia itself in cellulite appearance? So to try to explain the interaction in between layers we created the concept of skin envelope (SE). The skin envelope have a certain tension in between layers and against gravity, since we are born. With change of habits, BMI and ageing the tension and balance in between the layers change and some anatomical types of SE such as: man and women with no cellulite, are less affected by those changes. The reason is that their anatomical structure that gives resistancy to changes is weak. The ideal SE structure have enhanced amount of thick septae, thick layer of superficial fascia and septae distribution have a more perpendicular angle (90º) to the skin. The studies of Quelux clearly showed, with MRI of cellulite women compared with men and other women with no cellulite, 3 important things in cellulite patients: the superficial fascia is almost inexistent, the number of septaes is much smaller as is its thickeness, and the disposition os the septae is more oblique than perpendicular ( which would give less room for movement in between layers). So if we think that tension in between the layers fight against deformation of the surface (skin irregularities) we have to understand all factors involved in maintaining this tension to assess properly each case. The term skin irregularities was used by Cotofana and it is a good description of all we can find in cellulite patients. The tension is distributed in vectors and we will devided in three :
Vectors of Projection
- What – Projection is how much the area has projection towards the outside. It would be a 90º line against the gravity.
- Where – Structures involved: the deep fat layer, superficial fat layer, muscle mass and also the structural septae pulling.
- How – this is the most difficult vector to evaluate as there is no direct way of understanding how much it has been lost. The best way would be to compare pictures of 10 years before at least. Another tool is to measure the actual BMI and if it is below 20 most probably there will be a projection loss.Another way is evaluate the patient in standing position and look at the projection according to the body shape, also evaluate muscle tension in contraction to assess muscle mass according to age.
- Which – Procedures that can interfere with those layers will interfere in the projection of the area: cryolipolisys, mesotherapy for fat reduction, septae realease with manual or tissue-stabilized guided subcision, augmentation with injectables.
Vectors of Horizontal tension
- What – Horizontal tension is how much the area has force against horizontal forces and it is better assessed in dynamics. It would be a horizontal vector line against the gravity.
- Where – Structures involved: dermis, superficial fascia system ( septaes and superficial fascia).
- How – with the patient in standing position you push the region in a vertical manner or ask the patient to contract the muscle. If the appearance is much worse or if more skin irregularities, rippling, dimples appear that means there is horizontal loss.
- Which -Procedures that can interfere with those layers will interfere in the horizontal tension of the area : EBD for dermal tightening and injectables used as bioestimulators (PLLA, CaHA, HA).
Vectors of Vertical tension
- What – Vertical tension is how much the area has force directly against the gravity( counter-force) in a standing position. It would be a vertical vector line against the gravity.
- Where – Structures involved: dermis, superficial fascia system ( septaes and superficial fascia).
- How – with patient laying face up or down ( depending the area of evaluation) ask them to stand and observe what happens with the area involved. If skin irregularities worsen that means there is a loss in the vertical tension
- Which -Procedures that can interfere with those layers will interfere in the vertical tension of the area: microfocused ultrasound, EBD for fascia and septae tightening
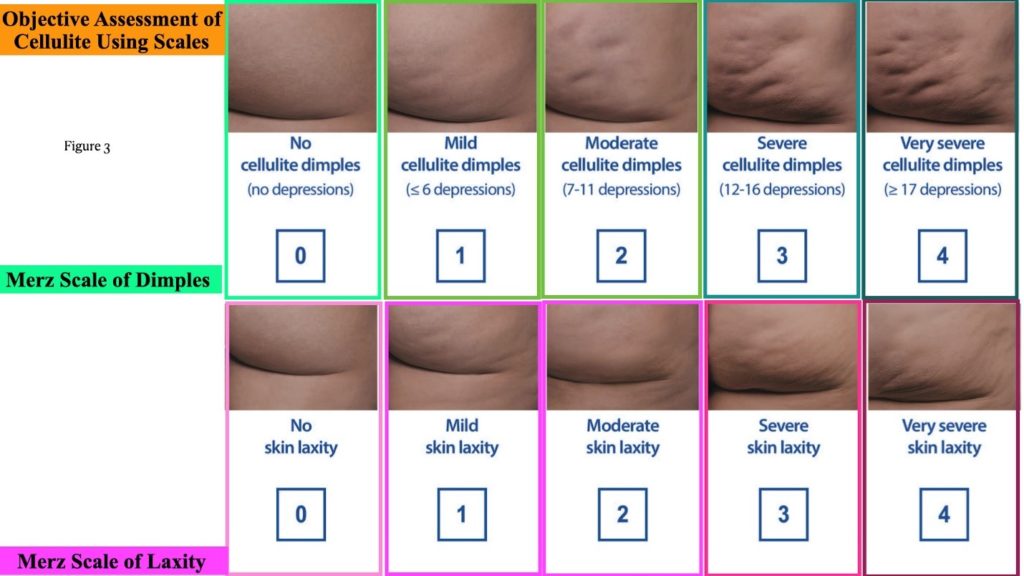
Scales and Severity (Figure 3)
Once the vectors are well know one have to decide how many sessions or how much product you need for the improvement. One objective way of identifying the answer for those questions is to use scales. Scales can give a good idea of severity and also estimate where the patient expect to get, in terms of improvement, with the procedure. There are scales available for cellulite grading. The authors recommend the use of at least 3 scales: one for dimple in rest, one for dimples in dynamic and one for laxity of the region. Another tool to evaluate profit of non-surgical procedures for cellulite is also to use the formula: Maximum BMI -Minimun BMI = X: 0<X<2 very good profit , 2<X<5 good profit, X>5 not good profit.
Treatments and complication
Energy Based Devices (EBD)
Radiofrequency (RF): (table 1) ( Figure 4, 10 a,b/ 12a,b)
The RF is a very common type of EBD used for the improvement of cellulite. The technology delivers heat to different layers of the skin and superficial subcutaneous fat. RF delivers heat through electrodes and the system can vary a lot. There are the monopolar and bipolar systems with or without suction, that were the first ones in the market, followed by multipolar and multigenerator and lately invasive temperature control electrode. It can also be associated with Infrared and electromagnetic pulse. The objective is to heat de dermal only or also superficial fat layers without any damage to the epidermis. Treatment temperature varies from 38 – 43 degrees which promotes neocollagenesis and neoelastogenesis through heat protein shock stimulation rather than coagulation of proteins. It can also promote lipolisys and apoptose of adipose cells depending on the depth and duration of treatment. The procedure is described to improve not only skin quality but also the superficial fat layer thickness, therefore improving tightness and decreasing the tension in SE. It is a good treatment for mild cases as a shock treatment and as an adjuvant treatment in moderate and severe cases. Among them, and newer in generation, is the subsurface minimally invasive RF that have a control of temperature. Unfortunately there are very few publications on the use,specifically, for cellulite improvement but the author believe it’s a promising and safe technology for tightening of SE. In the opinion of the authors “on the surface” RF are an excellent and indispensable tool for maintenance of results achieved.
Complications: The complications described with RF are rare. The most common one is burning and always technical dependent. The important step to avoid complications is to control temperature of the surface specially in cases of post operative areas or areas where the sensibility is diminished.
Protocol : Table 1
| Name – BRAND | TYPE OF RF | ASSOCIATION ( other technology associated ) | PROTOCOL |
| Venus Legacy (Venus Concept) | Multipolar | Succion and pulsed magnectic field | 1xweek 10 sessions |
| Exilis 360 (BTL) | Monopolar | no | 1x week 6 weeks |
| Velashape (Candela) | Bipolar | Infrared/ massage/ suction | 2x/week 6 weeks |
| Thermage ( Solta) | Monopolar | Vibration and cooling | 1 X year |
| ThermiRF | Bipolar | Invasive with temp. control | 1-2 sessions 3 months apart |
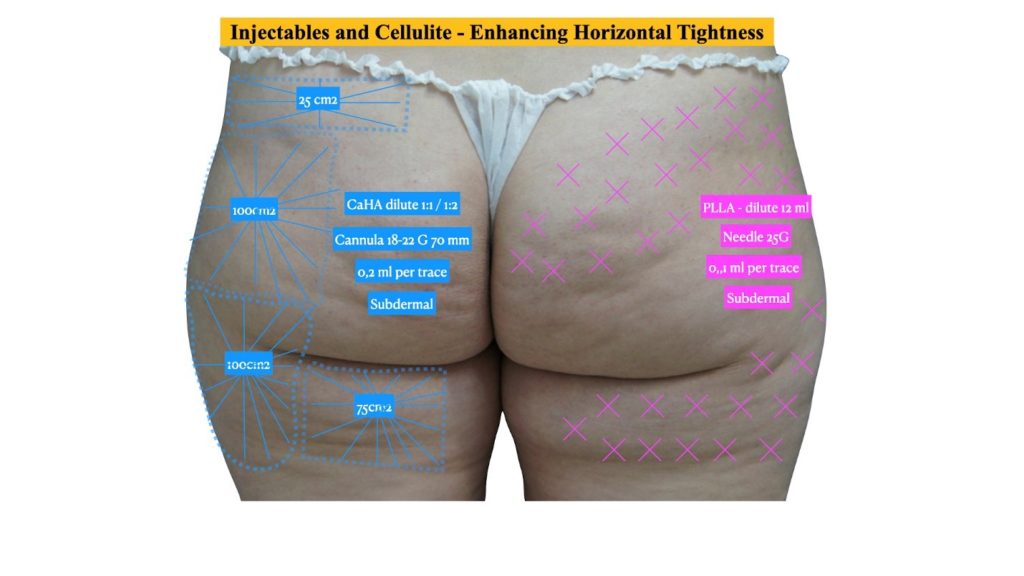


Figure 10. a. before and b. after RF weekly combined with injections CaHA dilute 1:1 combined with hyaluronic acid injected superficially non diluted.


Figure 12 a. before and b. after 3 months of 10 sessions of RF multipolar with vacuum weekly combined with LPG also weekly 10 sessions and mesotherapy and cryolipolysis on the lateral posterior thigh 1 session 1 aplicator per side.
NdYAG LASER (1440nm)
This laser is well absorbed by water and fat at the same time. The device is called Cellulaze (Cynosure) and use a 1,440-nm neodymium-doped yttrium aluminum garnet (Nd:YAG) laser therapy with a probe that is inserted under the skin targeting at the same time : superficial fat layer, superficial fascia system and dermis. It has to be done under tumescent anesthesia and the cannula has a real time temperature control to avoid overheating of the tissues. Is a quite new technologie and has demonstrated, in the few studies published, that it can offer 40-50% improvement in dimpling and 66-70% improvement in skin contour (thickness + appearance).
Complications: The most common complications is also burning and hyperpigmentation if the temperature of the surface get over 50ºC for some seconds.
Protocol : 1-2 sessions 6 weeks apart. Good for shock treatment.
Microfocused Ultrasound with Visualization ( MFU-V). ( Figure 4, 11a,b)
Microfocused ultrasound with visualization is a technology that induces thermal coagulation in 3 different layers : 4,5mm, 3,0mm and 1,5 mm. It is a predictable and very efficient tool to stimulate new collagen and elastin in the SE. AS we saw above the strength in the skin layer and also fascia layer play an important role in cellulite appearance. Casabona et al in 2017 showed that the combination of MFU-V and biostimulator with CaHA had a significant impact in cellulite in posterior thigh and gluteus. The target for cellulite patients is the deep dermal level, septae level and the deep SFS level. Most of the recommendations published use t only two layers ( 4,5 and 3,0mm) to treat but in the authors experience the use of the more superficial one (1,5mm) improve the skin laxity specially in more severe cases with laxity involved. The region to be treated is marked using a ruler ( 10X2,5 cm) and the number of lines decided per ruler / per transducer. The treatment do not require anesthesia and to decide the number of lines the severity scale is keen. The more severe the bigger the number of lines per ruler and the number of layers used. A patient that is a grade 1 in dimple scale but grade 3 in laxity scale will get more lines and layers per rules than one that is grade 2 in both.
Complications: All complications described are related to coupling and also spacing the lines. It can cause dermal burning if the device is not well coupled or 4,5 depth transducer delivered too superficial due to bad coupling or thick gel layer. Also the 1,5 mm transducer can also cause urticariform lines that, most commonly, last 1 week and respond well to topical esteroids but it can last up to 3 months.
Protocol : 1 session per year. Good to enhance vertical vector. 15-50 lines per ruler per transducer depending on severity.
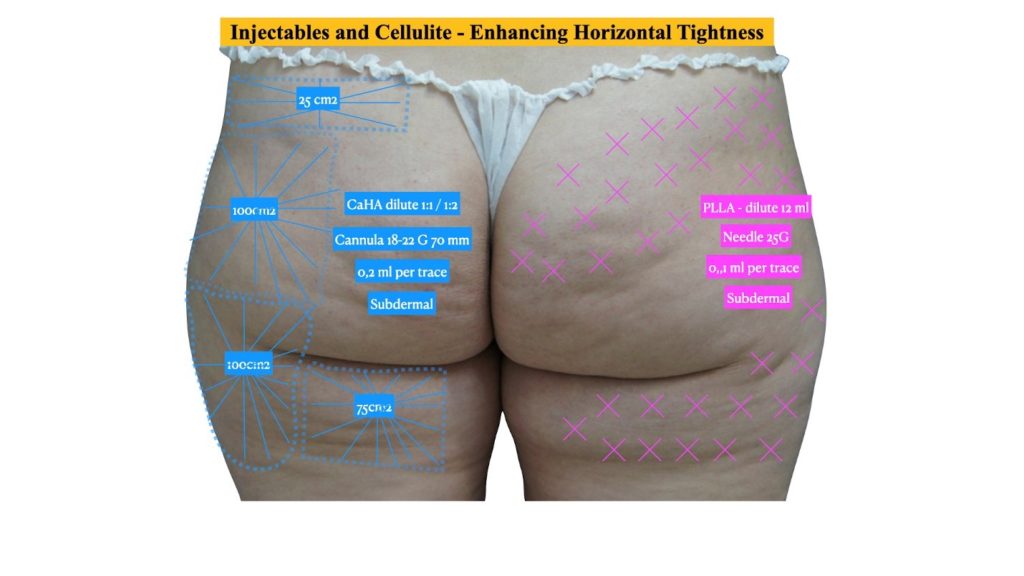




Figure 11 a,b before and c,d. after guided subcision 1 session combined with CaHA injections diluted 1:1, 1 syringe per side, 1 session a month later and same day MFU-V 550 lines
Acoustic shock waves
The acoustic shock waves were primarily used in orthopedic and urology to either to control pain or destroy kidney stones. Pressure waves are transmitted to the subcutaneous tissue and promote lipolysis, improve local blood flow, enable lymphatic drainage, and stimulate the production of new collagen. Two types of acoustic waves have been used to treat cellulite: focused shock waves (ESWT) (Cellactor, Storz) and radial shock waves (X Waves, BTL). The disadvantage is that the effects last as long as the patient is treating.
Complications: No complications described so far.
Protocol: 2 x week 4-6 weeks. Good as adjuvant for shock treatments in mild-severe cases and a wonderful choice for maintenance.
LPG and Manual Massage– (Figure 12a,b)
Massage as a treatment for cellulite is one of the oldest treatments described and had the idea to interact with the liquid accumulation explained above. Later on other devices were developed to improve the effectiveness of the massage adding vacuum to the equation, endermology, which means : a technique that uses suction ( negative pressure) to massage tissue. One of the first machines in the market was called LPG and has shown to be effective for a short time such as 12 weeks. The suction and pressure on the tissue showed to induce fibroblast to produce extracellular matrix and collagen and keratinocytes proliferation due to tensional stress, leading to a thicker epidermal/dermal layer, therefore enhancing tension SE. Also mechanical effect of pressure of the adipocytes not only cause disruption but also inhibits its differentiation reducing its size, therefore reducing pressure in the SE. It is used more as a maintenance treatment. (Level efficacy – high for grade 2, low BMI, young patients that has no evident skin laxity).
Complications: Bruising is the most common adverse event that normally resolves spontaneously in 1 week.
Protocol – once a week as maintenance treatment.


Figure 12 a. before and b. after 3 months of 10 sessions of RF multipolar with vacuum weekly combined with LPG also weekly 10 sessions and mesotherapy and cryolipolysis on the lateral posterior thigh 1 session 1 aplicator per side.
Cryolipolisys – ( Figure 8, 12 a,b )
Crylipolisys is a technologie that uses controlled cold ( -11ºC) to induce not only fat necrosys but also apoptosis ( atural death) of the adipocytes. It is used for fat accumulation and excess and a retrospective study in 2020 from Carruthers et al showed that can promote skin tightening in the region. As one of the main problems associated with the worsening of the cellulite appearance is accumulation of fat and higher pressure on the SFS the authors see as a good options for some regions such as : posterior thigh, abdomen, arms, to associate cryolipolisys to not only reduce superficial fat pressure but also induce skin tightening. The procedure would interfere with projection and vertical vectors.
Complications: The most common ones are mild to moderate such as : redness and pain that can last 1 week, bruising and edema that resolves spontaneously, hyperesthesia in the region that can last up to a month. There are very few descriptions of severe complications and the most common ones are : burning that depends on the technique and device used and fat hyperplasia that need to be treated with liposuction.
Protocol : 1-6 cicles , 1-2 sessions 3 months apart per area depending on the region.
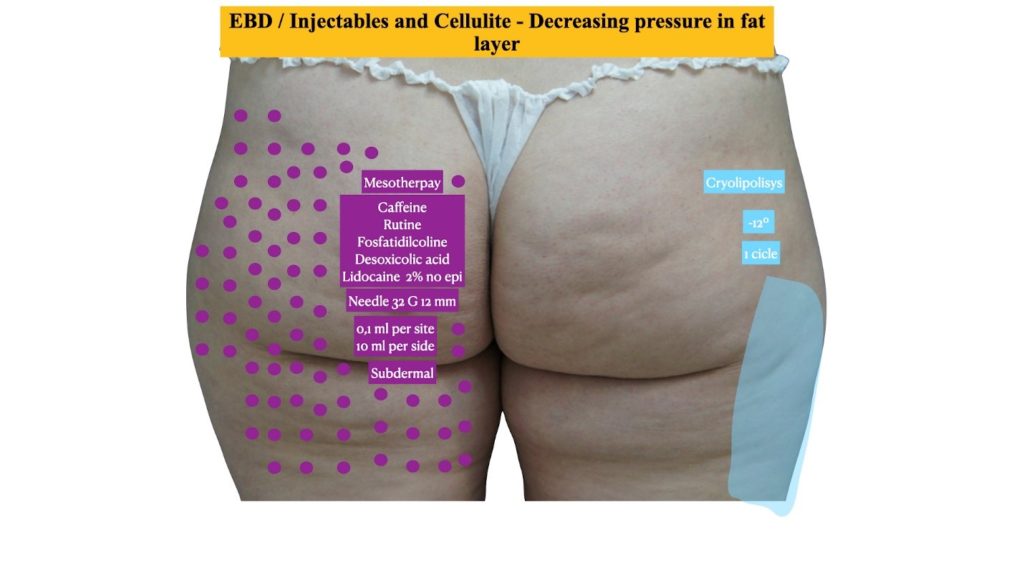


Figure 12 a. before and b. after 3 months of 10 sessions of RF multipolar with vacuum weekly combined with LPG also weekly 10 sessions and mesotherapy and cryolipolysis on the lateral posterior thigh 1 session 1 aplicator per side.
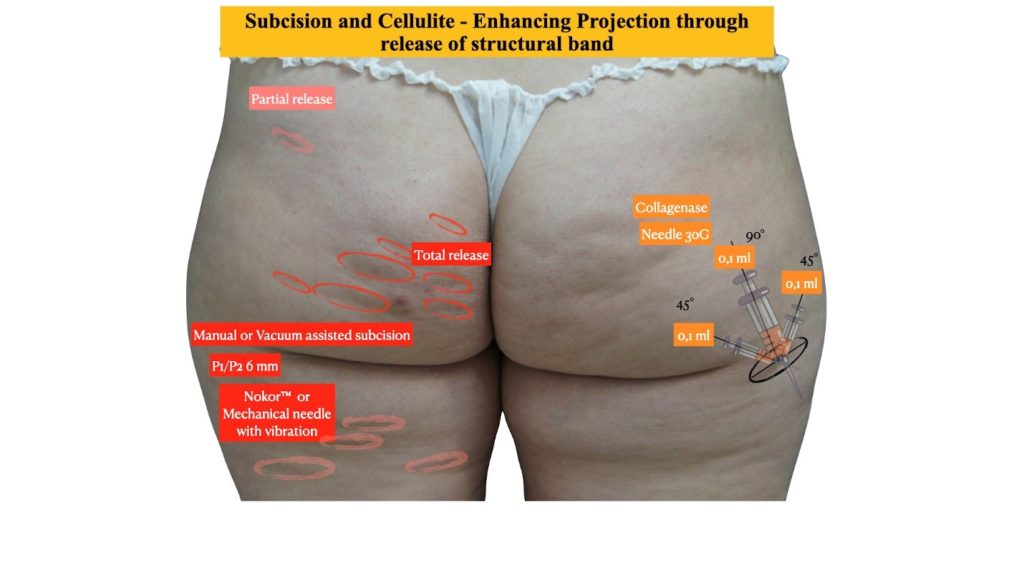
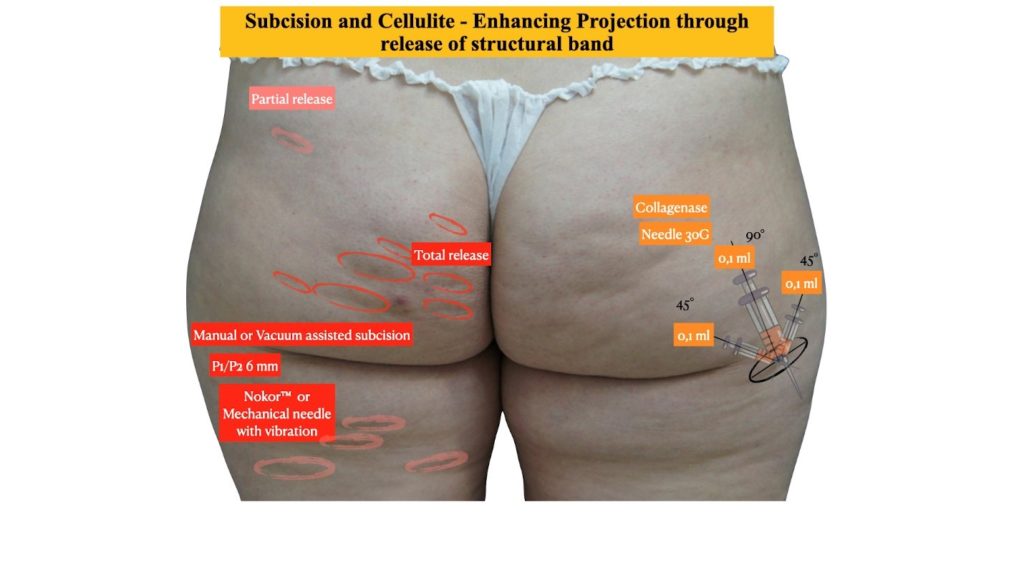
Subcision (Figure 7,11a,b)
Subcision was first described by Hexsel in 2000. It is a medical treatment that aim to release some of the structural bands that are one of the causes for the dimples, which are part of the appearance of cellulite. It was originally described to be done with special needle Nokor (BD) that has a blade on the tip. The needle is connected to a syringe of 10 ml, than inserted in the region and by moving the needle in subcutaneous plane, the blade would cut the band. In 2012 a mechanical subcision called Cabouchon was developed and than renamed as Celfina by Merz Pharmaceutical. It consists in vacuum assisted guided subcision (Figure A). Both methods have shown efficacy as stand-alone procedures or in combination with other procedures. Both procedures can be done under local anesthesia. The release of the bands should be carefully decided not to create full disconnection in between skin and deep fat layer ending up with an irreversible laxity of the gluteus or posterior thigh.
Complications: tha most common ones are mild such as : edema and bruising that can last up to 15 days. The most feared complications are the fat herniation and increase of laxity both related to over-release of septaes. Also infection has been described and should be treated with oral antibiotics.
Protocol – Manual = 1-3 sessions , 3 months apart/ Guided subcision = 1 session. Good for shock treatment of projection ( dimples and rippling are target)
Injectables
Bioestimulators
Calcium Hydroxyapatite (CaHA) ( Figure 3,5, 9a,b, 10a,b, 11a,b)
Calcium Hydroxyapatite (Radiesse ™, Merz, Germany) is a product used for volumization and bioestimulation since 2006. It has particles of CaHA, varying from 25-45 microns, embedded in a carbomimethylcellulose gel. It is used in a dilute form (1:1-1:4) for regeneration. Many studies already demonstrated its efficacy in bringing neocollagen and elastin to the skin level for rejuvenation purposes. One study demonstrated its use in the improvement of cellulite appearance through enhancement of laxity. The purpose was to bring better tightness in skin level and also in the superficial fascia system level, therefore enhancing the whole SE tension. Also this study compared different dilutions and showed that 1:1 and 1:2 dilutions stimulate much more collagen than others. The international consensus for CaHA use recommended, in 2017, that gluteal area should be injected with cannula or needle in subdermal plane respecting 100 cm2per syringe. In the authors experience the dilution 1:1 ( 1,5 ml CaHA + 1,5 ml lidocaine 2% no epi) should be used in low and normal BMI (15-22) patients and dilution 1:2 in patients with higher BMI (22-30) but with double amount of syringes per 100cm2 to maintain the same amount particles per area ( the more dilution the more diffusion of the product and less particles per area). This treatment is indicated for types …… where laxity is tone of the factors involved.
Complications: The most common adverse events are edema and bruising that resolve spontaneously. There is no moderate or severe complications described with CaHA diluted and the authors themselves had experienced none.
Protocol : 1-3 sessions /1 month apart , 1 syringe per 100cm2 (number of syringes may vary depending size of the total area)
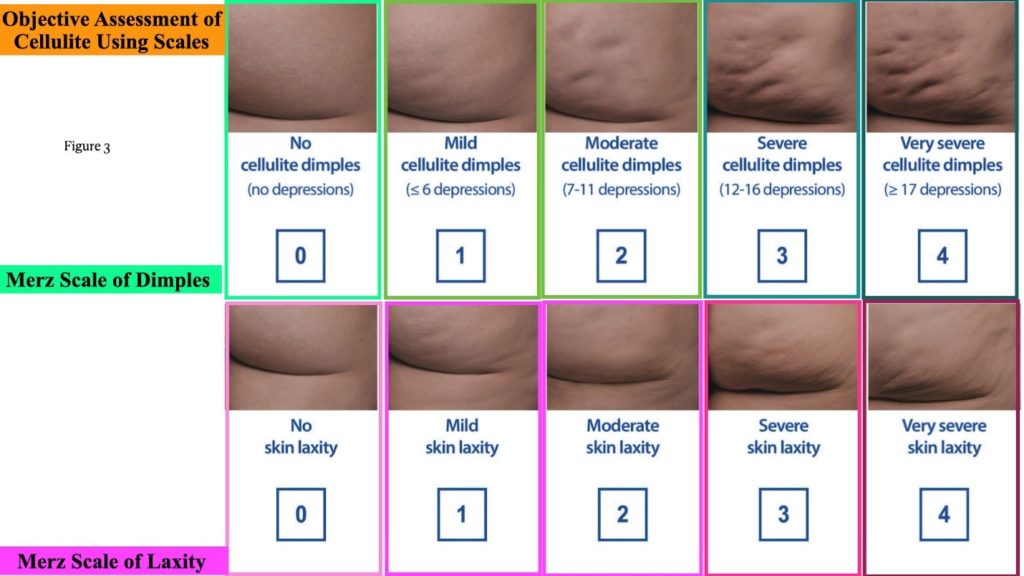
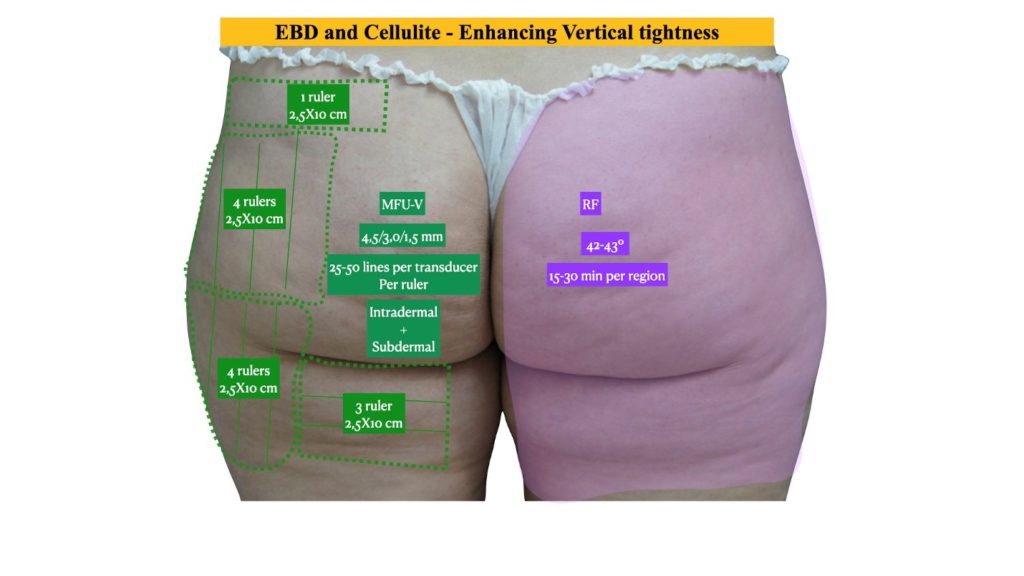


Figure 9 a. patient before and b. after 3 months of 2 sessions of CaHA injection diluted 1:1, 1 syringe 1,5 ml per side.


Figure 10. a. before and b. after RF weekly combined with injections CaHA dilute 1:1 combined with hyaluronic acid injected superficially non diluted.


Figure 11 a,b before and c,d. after guided subcision 1 session combined with CaHA injections diluted 1:1, 1 syringe per side, 1 session a month later and same day MFU-V 550 lines
Poli-lactic acid (PLLA) ( Figure 3,5)
Injectable poly-l-lactic acid (PLLA)(Sculptra™Aesthetic;
Galderma Pharma SA/Galderma SA,Lausanne, Switzerland) is a biodegradable, biocompatible and immunologically inert polymer derived from a group of alpha hydroxy acids. It was primarily used as a filler in 2004 by Vleggaar and currently mainly considered a biostimulator, since its main effect is neocollagenesis. In the year 2010 it started to be used in a more diluted form for body and facial laxity with the main purpose of stimulating collagen and in a more concentrated form to gain volume in certain regions such as gluteus. The consensus recommendation suggest dilution of PLLA to 10-20 ml final solution combining saline 0.9% 24hs prior to the injection and the rest added in the day of injection using lidocaine 2% no epi. The most performed technique is to inject with needle 30º to the skin subdermal plane in a crosshatch manner. The aim is to promote neocollagenesis in dermal and subdermal area and enhance skin support, therefore improve cellulite appearance.
Complications: AS any injectable edema and bruising are the most common findings after a procedure. There are also some publication mentioning granulomas but those are more frequent when less diluted PLLA is used.
Protocol : 1-3 vials per session ( depending on area)/ month, 2-3 sessions. Good for pacients with low BMI associated with laxity
Collagenase ( Figure 7)
Collagenase clostridium histolyticum-aaes (CCH) is an enzyme that degrades collagen fibers. It enzymatically releases fibrous septa that contribute to the skin dimpling characteristic of cellulite. It is recommended only for well-defined dimples in rest position. It is injected with a 30 gauge needle 90 degree in the center of the dimple 0,1 ml followed by 45 degrees lateral to the first one from same point of injection again 0,1 ml both sides ( figure B)
Complications: Edema and bruising are the mlst common ones and resolve spontaneously.
Protocol: 3-6 sessions /a month apart/ 3,6 ml ( 0,84 mg) per session. Good indication for cellulite with no skin laxity involved as stand alone or in combination with other shock treatments.
Mesotherapy (Figure 8,12a,b)
Mesotherapy is a technique developed and first described by Pistor, a French doctor in 1952, who tried to inject procaine using intradermal small injections. Since than the technique has been used but not well accepted in all countries due to regulatory problems. Unfortunatelly there are very scarce publications on the technique used for cellulite improvement, in the experience of the author of 19 years using the technique, it is an easy and safe procedure to add on cases where there is a more edematous fat associated with mild skin laxity and fat herniation. There are innumerous active ingredients to be combined to form the Melange, which means the mixing agents, for injection. There are some countries that approved already made melanges such as Alydia ( Ghimas,Italy) or Mesoestetic ampoules for mesotherapy (Mesoestetic, Spain).The most common ones are: pentoxiphylline (vasodilator), hyaluronidase (enhance diffusion), collagenase ( destroy excess collagen in septae), carnitine ( enhance fat metabolism), calcium pyruvate, aminophylline ( enhance AMP cyclic and local metabolism), caffeine (enhance AMP cyclic and local metabolism), coumarin (vasodilator and antiinflamatory), artichoke and melilotus (enhance local drainage), phosphatidylcholines (PC) and desoxycholate (DC) ( both promote fat reduction by different mechanisms)
Main Melanges :
- Fat reduction – PC/ DC 2 ml diluted with 8 ml liidocaine no epi and aminophylline / caffeine 2ml + hyaluronidase 2ml + carnitine 2ml + artichoke and melilotus 2 ml + lidocaine 2 ml
- Reduce edema – hyaluronidase 2ml+ artichoke 2 ml + melilotus 2 ml+ pentoxiphylline 2ml + 2 ml lidocaine
- Structural bands – collagenase 4 ml + hyaluronidase 2ml + lidocaine 2 ml
The area is injected respecting 2 cm in between the points of injection and using 30G or 32G needle 4-8mm ( depending on the layer you want to deposit dermal only or intradermal + subcutaneous) 30º to the skin and 0,2 ml each point of injection.
Complications: Apart from edema and bruising which are very common the complications are rare but sometimes also severe. The severe complications can go from local allergy, infection that can be caused most commonly by gram + or mycobacterias. The important step to avoid this is to do a good medical history and also to control the storage and origin of the active ingredients.
Protocol : Melange 10 ml per side – 1 sessions a week = 10 sessions, maintenance 1 sessions 15/15 days for 3 months. Good for shock treatment combined with other procedures. There is a disadvantage that the results last while the patient is being treated and maintained.
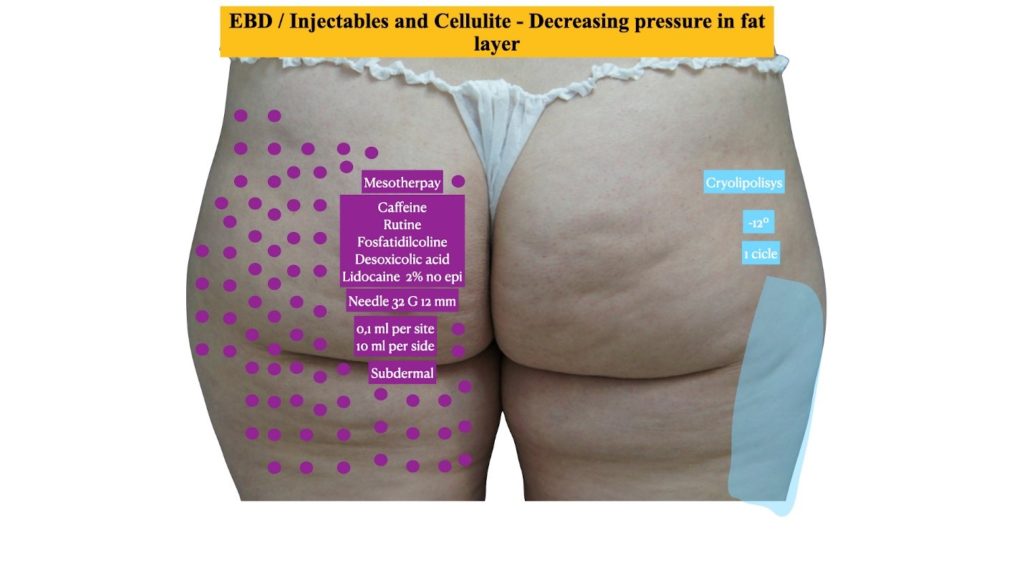


Figure 12 a. before and b. after 3 months of 10 sessions of RF multipolar with vacuum weekly combined with LPG also weekly 10 sessions and mesotherapy and cryolipolysis on the lateral posterior thigh 1 session 1 aplicator per side.
Oral
The goal of the oral medications against cellulite are distributed in two main groups : induce drainage of liquid accumulation and induce thermogenesis (
loss fat through enhancing fat metabolism)
- Thermogenic effect:
- CLA or …. is a peroxisome proliferator-activated receptors (PPAR) agonist and affect mainly the skin homeostasis by activating proliferation of keratinocytes and dermal thickening and adipocyte therefore will have an effect in the epidermal/dermal and the superficial fat component. The recommendation is to use as a long term treatment. Dose : 800mg / day ( min 90 days)
- Asiatic Centella -is another PPAR agonist. The main effect demonstrated in studies are in reducing fat layer by reducing size of adipocytes and also the fibrosis existing in fat layer. Dose : 60 mg / day ( min 90 days )
- Garcinia cambogia – also a PPAR agonist. Mostly studied for weight control but very common used in combination with other herbs to reduce adipogenesis and reduce adipocyte size. Dose …
- Green Tea – is a strong PPAR agonist and although it has not been published for the use in cellulite yet it has been studied as an adjuvant for weight loss or control. As any interference in fat layer pressure improve cellulite its logical that it will have an effect in cellulite patients. Dose:
- Diuretic effect
Topical
Although the idea of topical cream or lotion that can improve cellulite have been marketed for a long time the efficacy of those products is limited. As Welcher showed in 2012 the efficacy of an active ingredient depends not only on the concentration on the surface but also capacity of penetration, particle size and vehicle used. So the perfect drug delivery system that can achieve maximum efficacy is still to come. The main active ingredients used in the creams are :
-Methylxanthynes ( caffeine, aminophilline and theofilline) are commonly used and are expected to induce lipolysis through inhibiton of phosphodiesterase and enhancing metabolism through amino phosphoesterase (AMP).
Retinoic Acid (RA) – The RA can bind to different receptor in a cell membrane therefore can stimulate the nucleous in different ways. Its main effect is to induce improvement of fibroblast function, neocollagenesis, extracellular matrix production and keratinocytes proliferation. Also it induce a reduction in adipogenesis through enhanced mitochondrial coupling proteins (free proteins present in nucleus that stimulate metabolism to generate heat) therefore enhanced cellular heat dissipation. Its been shown to have in a long term use an impact in two layers of SE : the dermal/epidermal component explained by the thickening promoted and superficial fat .layer component by modulating adipogenesis. Dose : 0,3-1% in cream combined or not with methylxantynes and centella asiatica.
Herbal : Most of the studies published show some improvement with the use of creams containing active herbal ingredients but all of the publications use combination of 3 or more ingredients which make it difficult to know if there is a specific role of one ingredient alone on the improvement seen. The herbal combinations that showed significant improvement in stand alone treatments are:
- verbena, green tea, lemon, kola nut,fennel, algae, ivy, barley, strawberry, marjoram, sweet clover
- caffeine, horsechestnut, ivy, algae, bladderwrack, plankton, butcherbroom and soy protein
- black pepper, sweet orange peel, ginger root extract, cinnamon bark extract, capsaicin, green tea and caffeine
- hydroglycolic gel containing extracts of Terminalia seracea, Visnaga vera, Plectreinthus barbatus and Cola lipa together with cyclic AMP
FINAL REMARKS
What is important to highlight here is that there is not “one do it all” treatment for this condition. Unfortunately, because of its multilevel cause, many times the answer is a combination of shock treatments followed by maintenance. Our body ageing is dynamic as much as our restoration. Our skin cells renovate, our fat cells change, our fascia system age therefore there is a chance to improve and change the course of cellulite every day but it will almost always be a lifetime treatment.
LEGENDS
Figure 1 Skin envelope in a. women and b. men
Figure 2 Types of cellulite according to scale grading and also fat accumulation grading
Figure 3 How to use the scales to grade cellulite patients
Figure 4 Enhancing Horizontal vector with injectables
Figure 5 Enhancing Vertical vectors with EBD
Figure 6 Enhancing Projection with injectables
Figure 7 Enhancing Projection with release structural bands
Figure 8 Decreasing fat pressures and projection with Cryolipolisis and mesotherapy
Figure 9 a. patient before and b. after 3 months of 2 sessions of CaHA injection diluted 1:1, 1 syringe 1,5 ml per side.
Figure 10. a. before and b. after RF weekly combined with injections CaHA dilute 1:1 combined with hyaluronic acid injected superficially non diluted.
Figure 11 a,b before and c,d. after guided subcision 1 session combined with CaHA injections diluted 1:1, 1 syringe per side, 1 session a month later and same day MFU-V 550 lines.
Figure 12 a. before and b. after 3 months of 10 sessions of RF multipolar with vacuum weekly combined with LPG also weekly 10 sessions and mesotherapy and cryolipolysis on the lateral posterior thigh 1 session 1 aplicator per side.
REFERENCES
- Rudolph C, Hladik C, Hamade H, Frank K, Kaminer MS, Hexsel D, Gotkin RH, Sadick NS, Green JB, Cotofana S. Structural Gender Dimorphism and the Biomechanics of the Gluteal Subcutaneous Tissue: Implications for the Pathophysiology of Cellulite. Plast Reconstr Surg. 2019 Apr;143(4):1077-1086. doi: 10.1097/PRS.0000000000005407. PMID: 30730492.
- Goldman, M.P. Cellulite: a review of current treatments. Cosmet. Dermatol. 15, 17–20 (2002).
- Pierard, G.E., Nizet, J.L. and Pierard-Franchimont, C. Cellulite: from standing fat herniation to hypodermal stretch marks. Am. J. Dermatopathol. 22, 34–37 (2000).
- Querleux, B., Cornillon, C., Jolivet, O. and Bittoun, J. Anatomy and physiology of subcutaneous adipose tissue by in vivo magnetic resonance imaging and spectroscopy: relationships with sex and presence of cellulite. Skin Res. Technol. 8, 118–124 (2002).
- Rawlings AV. Cellulite and its treatment. Int J Cosmet Sci. 2006 Jun;28(3):175-90. doi: 10.1111/j.1467-2494.2006.00318.x. PMID: 18489274.
- Mirrashed, F., Sharp, J.C., Krause, V., Morgan, J. and Tomanek, B. Pilot study of dermal and subcutaneous fat structures by MRI in individuals who differ in gender, BMI, and cellulite grading. Skin Res. Technol. 10, 161–168 (2004).
- Callaghan, T. Evaluating cellulite – reality redirecting the dream to dispel the myth. Proceedings International Federation of the Society of Cosmetic Chemists (IFSCC), Orlando, FL (2004).
- Adcock, D., Paulsen, S., Jabour, K., Davis, S., Nanney, L.B. and Shack, R.B. Analysis of the effects of deep mechanical massage in the porcine model. Plast. Reconstr. Surg. 108, 233–240 (2001).
- Tanabe, Y., Koga, M., Saito, M., Matsunaga, Y. and Nakayama, K. Inhibition of adipocyte differentiation by mechanical stretching through ERK-mediated downregulation of PPARgamma2. J. Cell. Sci. 117, 3605–3614 (2004).
- Wiechers, J.W., Kelly, C.L., Blease, T.G. and Dederen, J.C. Formulating for efficacy. Int. J. Cosmet. Sci. 26, 173–182 (2004).
- Wiechers JW, Watkinson AC, Cross SE, Roberts MS. Predicting skin penetration of actives from complex cosmetic formulations: an evaluation of inter formulation and inter active effects during formulation optimization for transdermal delivery. Int J Cosmet Sci. 2012 Dec;34(6):525-35. doi: 10.1111/ics.12001. Epub 2012 Oct 11. PMID: 22950455.
- Hexsel, D., Orlandi, C. and Zechmeister do Prado, D. Botanical extracts used in treatment of cellulite. Dermatol. Surg. 31, 866 872 (2005).
- Buscaglia, D.A. and Conte, E.T. The treatment of cellulite with methylxanthine and herbal extract based cream: an ultrasonographic analysis. Cosmet. Dermatol. 9, 30–40 (1996).
- Rao, J., Paabo, K.E. and Goldman, M.P. A double-blinded randomized trial testing the tolerability and efficacy of a novel topical agent with and without occlusion for the treatment of cellulite: a study and review of the literature. J. Drugs Dermatol. 3, 417–425 (2004).
- Kligman, A.M., Pagnoni, A. and Stoudemayer, T. Topical retinol improves cellulite. J. Dermatol. Treat. 10, 119–125 (1999).
- Pierard-Franchimont, C., Pierard, G.E., Henry, F., Vroome, V. and Cauwenbergh, G. A randomized, placebocontrolled trial of tropical retinol in the treatment of cellulite. Am. J. Clin. Dermatol. 1, 369–374 (2000).
- Gaullier, J.M., Halse, J., Hoye, K. et al. Conjugated linoleic acid supplementation for 1 y reduces body fat mass in healthy overweight humans 1–3. Am. J. Clin. Nutr. 79, 1118–1125 (2004).
- Lee, K. Transactivation of peroxisome proliferators activated receptor alpha by green tea extracts. J. Vet. Sci. 5, 325–330 (2004).
- Angehrn F, Kuhn C, Voss A. Can cellulite be treated with low-energy extracorporeal shock wave therapy? Clin Interv Aging. 2007;2(4):623-30. doi: 10.2147/cia.s1721. PMID: 18225463; PMCID: PMC2686339.
- Nassar AH, Dorizas AS, Shafai A, Sadick NS. A randomized, controlled clinical study to investigate the safety and efficacy of acoustic wave therapy in body contouring. Dermatol Surg 2015;41(3):366–70.
- Bartsch R, Casabona G, Sitzwohl C, Kimberger O, Green JB, Stanger J, Frank K, Onishi EC, Cotofana S. The Influence of Different Treatment Combinations on Skin Laxity and Dimpling. J Drugs Dermatol. 2020 Nov 1;19(11):1030-1038. doi: 10.36849/JDD.2020.5117. PMID: 33196744.
- Hexsel D, Dal Forno T, Hexsel C, Schilling-Souza J, Naspolini Bastos F, Siega C, Dal Forno T, Hexsel C, Naspolini Bastos F. Magnetic Resonance Imaging of Cellulite Depressed Lesions Successfully Treated by Subcision. Dermatol Surg. 2016 May;42(5):693-6. doi: 10.1097/DSS.0000000000000679. PMID: 27082058.
- Kaufman-Janette JA, Bass LS, Xiang Q, McLane MP, Kirby MT, Vijayan S. Efficacy, Safety, and Durability of Response of Collagenase Clostridium Histolyticum-aaes for Treating Cellulite. PlastReconstr Surg Glob Open. 2020;8(12):e3316. Published 2020 Dec 23. doi:10.1097/GOX.0000000000003316
- Goldie K, Peeters W, Alghoul M, Butterwick K, Casabona G, Chao YYY, Costa J, Eviatar J, Fabi SG, Lupo M, Sattler G, Waldorf H, Yutskovskaya Y, Lorenc P. Global Consensus Guidelines for the Injection of Diluted and Hyperdiluted Calcium Hydroxylapatite for Skin Tightening. Dermatol Surg. 2018 Nov;44 Suppl 1:S32-S41. doi: 10.1097/DSS.0000000000001685. Erratum in: Dermatol Surg. 2019 Feb;45(2):327. PMID: 30358631.
- Casabona G, Pereira G. Microfocused Ultrasound with Visualization and Calcium Hydroxylapatite for Improving Skin Laxity and Cellulite Appearance. Plast Reconstr Surg Glob Open. 2017 Jul 25;5(7):e1388. doi: 10.1097/GOX.0000000000001388. PMID: 28831339; PMCID: PMC5548562.
- Vleggaar D, Bauer U. Facial enhancement and the European experience with Sculptra (poly-l-lactic acid). J Drugs Dermatol. 2004 Sep-Oct;3(5):542-7. PMID: 15552606.
- Lorenc ZP. Techniques for the optimization of facial and nonfacial volumization with injectable poly-l-lactic acid. Aesthetic Plast Surg. 2012 Oct;36(5):1222-9. doi: 10.1007/s00266-012-9920-3. Epub 2012 Aug 28. PMID: 22926148.
- – Vleggaar D, Fitzgerald R, Lorenc ZP, Andrews JT, Butterwick K, Comstock J, Hanke CW, O’Daniel TG, Palm MD, Roberts WE, Sadick N, Teller CF. Consensus recommendations on the use of injectable poly-L-lactic acid for facial and nonfacial volumization. J Drugs Dermatol. 2014 Apr;13(4 Suppl):s44-51. PMID: 24719078
- Haddad A, Menezes A, Guarnieri C, Coimbra D, Ribeiro E, Sarubi J, Avelar LE, Del Nero MP, da Cunha MG, Mazzuco R, Kamamoto C, Cazerta C. Recommendations on the Use of Injectable Poly-L-Lactic Acid for Skin Laxity in Off-Face Areas. J Drugs Dermatol. 2019 Sep 1;18(9):929-935. PMID: 31524350.
- Mazzuco R. Subcision™ plus poly-l-lactic acid for the treatment of cellulite associated to flaccidity in the buttocks and thighs. J Cosmet Dermatol. 2020 May;19(5):1165-1171. doi: 10.1111/jocd.13364. Epub 2020 Mar 16. PMID: 32176410.
- Kaminer MS, Casabona G, Peeters W, Bartsch R, Butterwick K, Yen-Yu Chao Y, Costa J, Eviatar J, Fabi SG, Geister TL, Goldie K, Grice J, Hexsel D, Lorenc P, Lupo M, Pooth R, Sattler G, Waldorf HA, Yutskovskaya Y, Kerscher M. Validated Assessment Scales for Skin Laxity on the Posterior Thighs, Buttocks, Anterior Thighs, and Knees in Female Patients. Dermatol Surg. 2019 Aug;45 Suppl 1:S12-S21. doi: 10.1097/DSS.0000000000001994. PMID: 31246868.
- Hexsel D, Fabi SG, Sattler G, Bartsch R, Butterwick K, Casabona G, Yen-Yu Chao Y, Costa J, Eviatar J, Geister TL, Goldie K, Grice J, Kerscher M, Lorenc P, Lupo M, Peeters W, Pooth R, Waldorf HA, Yutskovskaya Y, Kaminer MS. Validated Assessment Scales for Cellulite Dimples on the Buttocks and Thighs in Female Patients. Dermatol Surg. 2019 Aug;45 Suppl 1:S2-S11. doi: 10.1097/DSS.0000000000001993. PMID: 31246867.
- Conti G, Zingaretti N, Amuso D, Dai Prè E, Brandi J, Cecconi D, Manfredi M, Marengo E, Boschi F, Riccio M, Amore R, Iorio EL, Busato A, De Francesco F, Riccio V, Parodi PC, Vaienti L, Sbarbati A. Proteomic and Ultrastructural Analysis of Cellulite-New Findings on an Old Topic. Int J Mol Sci. 2020 Mar 18;21(6):2077. doi: 10.3390/ijms21062077. PMID: 32197394; PMCID: PMC7139738.
- Khan MH, Victor F, Rao B, Sadick NS. Treatment of cellulite: Part II. Advances and controversies. J Am Acad Dermatol. 2010 Mar;62(3):373-84; quiz 385-6. doi: 10.1016/j.jaad.2009.10.041. PMID: 20159305.
- Hexsel D, Camozzato FO, Silva AF, Siega C. Acoustic wave therapy for cellulite, body shaping and fat reduction. J Cosmet Laser Ther. 2017 Jun;19(3):165-173. doi: 10.1080/14764172.2016.1269928. Epub 2017 Feb 2. PMID: 27997260.
- Geronemus RG, Kilmer SL, Wall SH Jr, Green JB, Cohen JL, Weiss RA, Alster TS, Kaminer MS, Gupta A. An Observational Study of the Safety and Efficacy of Tissue Stabilized-Guided Subcision. Dermatol Surg. 2019 Aug;45(8):1057-1062. doi: 10.1097/DSS.0000000000001911. PMID: 30893161.
- Davis DS, Boen M, Fabi SG. Cellulite: Patient Selection and Combination Treatments for Optimal Results-A Review and Our Experience. Dermatol Surg. 2019 Sep;45(9):1171-1184. doi: 10.1097/DSS.0000000000001776. PMID: 30913048.
- Bass LS, Kaminer MS. Insights Into the Pathophysiology of Cellulite: A Review. Dermatol Surg. 2020 Oct;46 Suppl 1(1):S77-S85. doi: 10.1097/DSS.0000000000002388. PMID: 32976174; PMCID: PMC7515470.
- Amore R, Amuso D, Leonardi V, Sbarbati A, Conti G, Albini M, Leva F, Terranova F, Guida A, Gkritzalas K, Gavashely L, Velichenko R. Treatment of Dimpling from Cellulite. Plast Reconstr Surg Glob Open. 2018 May 18;6(5):e1771. doi: 10.1097/GOX.0000000000001771. PMID: 29922557; PMCID: PMC5999441.
- Pistor M. Qu’est-ce que la mésothérapie? [What is mesotherapy?]. Chir Dent Fr. 1976 Jan 21;46(288):59-60. French. PMID: 1076080.
- González-Suárez A, Gutierrez-Herrera E, Berjano E, Jimenez Lozano JN, Franco W. Thermal and elastic response of subcutaneous tissue with different fibrous septa architectures to RF heating: numerical study. Lasers Surg Med. 2015 Feb;47(2):183-95. doi: 10.1002/lsm.22301. Epub 2015 Feb 4. PMID: 25651998.
- Alexiades M, Munavalli G, Goldberg D, Berube D. Prospective Multicenter Clinical Trial of a Temperature-Controlled Subcutaneous Microneedle Fractional Bipolar Radiofrequency System for the Treatment of Cellulite. Dermatol Surg. 2018 Oct;44(10):1262-1271. doi: 10.1097/DSS.0000000000001593. PMID: 30222637.
- Sylwia M, Krzysztof MR. Efficacy of intradermal mesotherapy in cellulite reduction – Conventional and high-frequency ultrasound monitoring results. J Cosmet Laser Ther. 2017 Oct;19(6):320-324. doi: 10.1080/14764172.2017.1334927. Epub 2017 Jun 7. PMID: 28590783.
- Sivagnanam G. Mesotherapy – The french connection. J Pharmacol Pharmacother. 2010 Jan;1(1):4-8. doi: 10.4103/0976-500X.64529. PMID: 21808584; PMCID: PMC3142757.
- Carruthers J, Stevens WG, Carruthers A, Humphrey S. Cryolipolysis and skin tightening. Dermatol Surg. 2014 Dec;40 Suppl 12:S184-9. doi: 10.1097/DSS.0000000000000229. PMID: 25417573.
- Alizadeh Z, Halabchi F, Mazaheri R, Abolhasani M, Tabesh M. Review of the Mechanisms and Effects of Noninvasive Body Contouring Devices on Cellulite and Subcutaneous Fat. Int J Endocrinol Metab. 2016 Jul 3;14(4):e36727. doi: 10.5812/ijem.36727. PMID: 28123436; PMCID: PMC5236497.