Anatomy – Sex Differences and Aging of Jawline
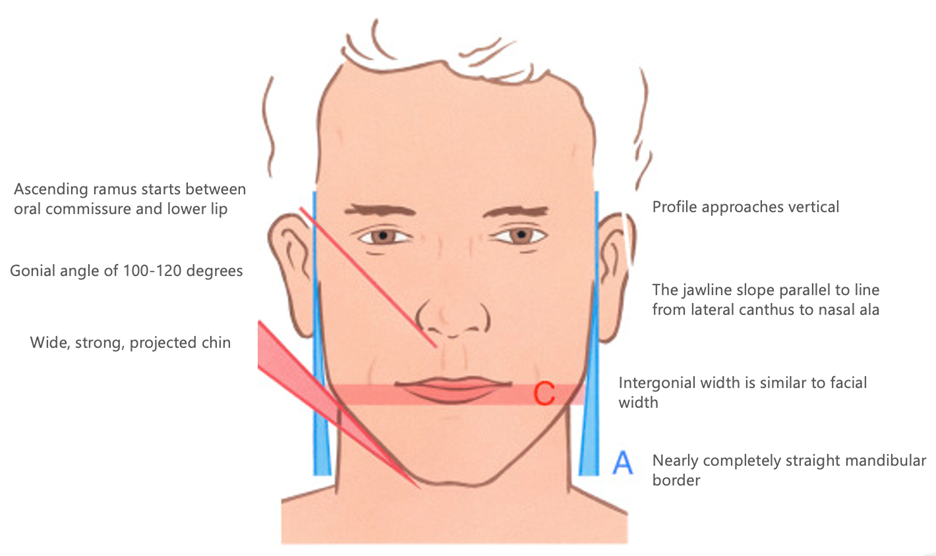
There are well document sexual dimorphisms of the ideal profile and jawline. Females tend to have slim lower faces with the bigonial width (width of the jaw) always less than the bizygomatic width (width of the cheeks). However, there is a wide range of widths which are still considered attractive. For instance, Angelina Jolie has a very wide bigonial width, yet she is still considered one of the most attractive female celebrities. Conversely, Gigi Hadid and Kendall Jenner, both have very narrow bigonial widths, giving a V-shaped face to the lower face, and are 2 of the most sought-after models in the industry. Ideally, males have very wide lower faces where the bigonial width is equal to the bizygomatic width. Additionally, large masseters and bulging temples are a sign of strength and masculinity.
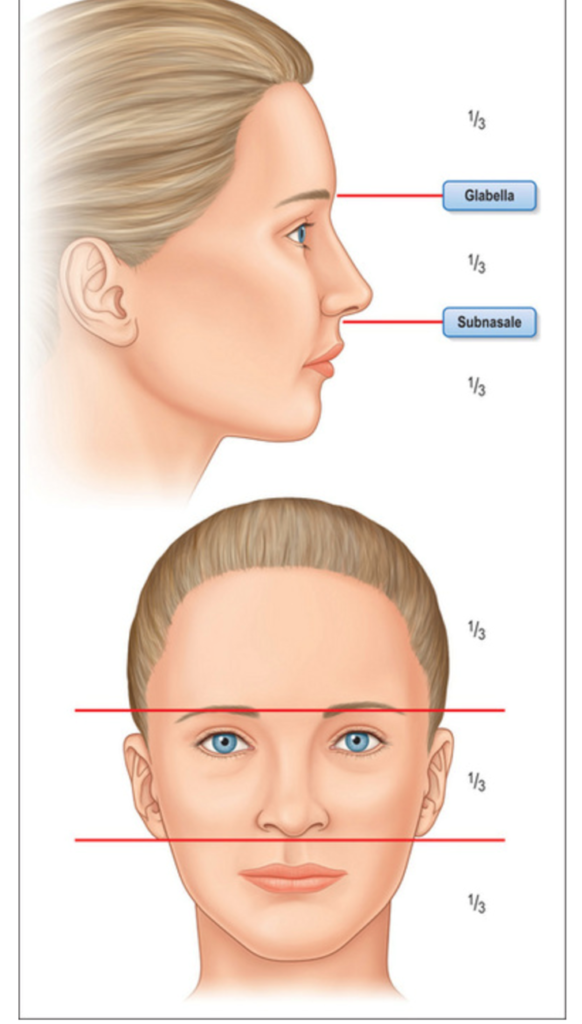
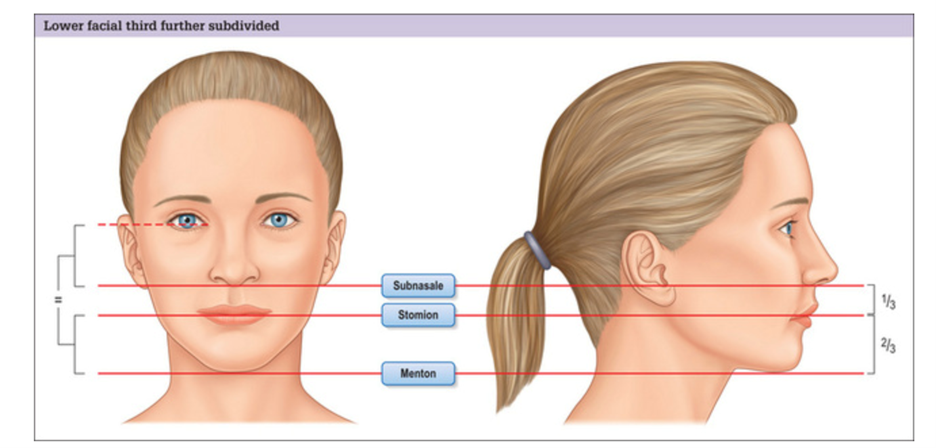
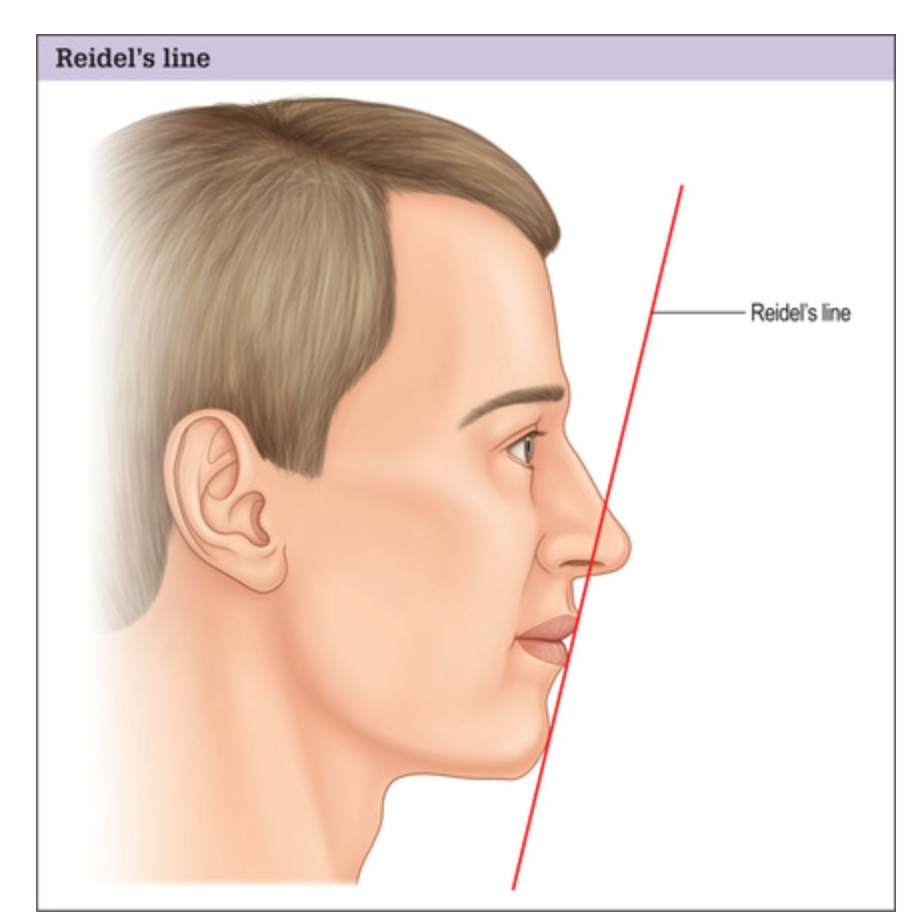
Chin width, projection, and length must be considered when addressing the lower face and jawline. The female chin must be narrow and projected. The width should be no wider than the width of the nose. In males, chin width is equal to the distance between the inner canthi. The perfect projection can be predicted using the Rickett’s E-Plane, Steiner’s S-Line or Reidel’s Line. The position of the menton (the most inferior portion of the chin) should follow the facial thirds and the distance from the stomion to the menton should be twice the distance from the subnasale to the stomion. (3) There should be one dominant point on a female and 2 on the male chin.
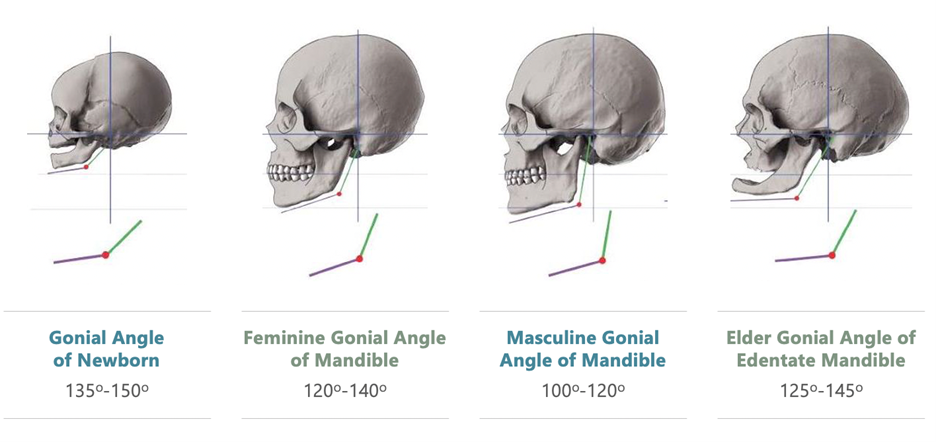
The gonial angle of a female is between 120-140 degrees and for the male it is 100-120 degrees. This angle should be on the same horizontal plane as the oral commissure in males, and in females, this plane is at the level of the upper lip. The height of the mandibular body is greater in males verses females and the ramus is more substantial in males vs females. (4,5)
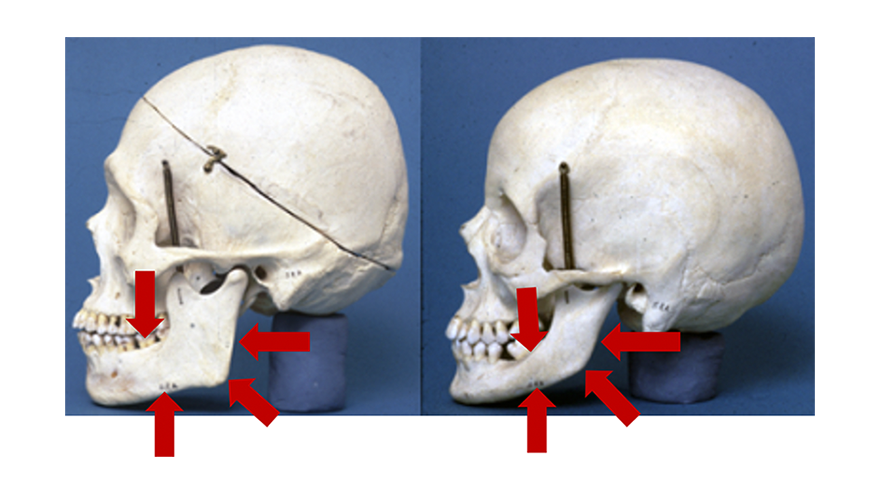
Aging of the jawline affects all layers of the lower face. The skin loses collagen and elastin. Superficial fat pads (Lateral Temporal Cheek, Superior and Inferior Jowl, Superficial Chin) are tightly adherent to the SMAS and descend with age. In particular, the lateral temporal cheek fat pad obscures the gonial angle and the retromandibular fossae. The platysma becomes hypertrophied and creates a negative vector affecting the jawline. The mandibular osseocutaneous and platysma mandibular ligaments are proposed to lose support. The deep fat pads, adherent to the periosteum, gradually lose volume.
The most significant age-related jawline changes occur at the level of the boney mandible. There is an overall general loss of bone throughout. The gonial angle resorbs and becomes more obtuse. The body of the mandible loses height, most notably in the edentulous patients. There appears to be deepening of the antegonial notch. The boney chin changes are widening and retrusion.
The clinical correlation to the age related phenomenon noted above is jowling, lower face widening, blurring of the distinction of the mandibular border and the neck, blunting of the gonial angle, loss of the shadow in the retromandibular fossae, and widening of chin with loss of projection.

Jawline Treatment Options
There are 2 distinct techniques for “reJAWvenation” depending on whether enhancement and restoration is the goal. Enhancement is reserved for the patient with minimal to no signs of aging who desires a more defined jawline and is generally age 40 or younger. The restoration reJAWvenation is performed on the aging jawline with overt jowling and other clinical signs of aging which were mentioned previously. Obviously, restoration is more clinically challenging to correct and most often requires multimodalities for optimal results.
The available treatments for the jawline include:
- Fillers
- Neuromodulators
- Deoxycholic Acid
- Radiofrequency including Radiofrequency Microneedling
- Lasers – Ablative and Nonablative
- Thread Lifting
- Liposuction
- Surgery
reJAWvenation is a nonsurgical approach to enhancement and restoration of the jawline. The technique is a quick, minimal downtime procedure with instantaneous results using fillers. Not all patients will benefit from fillers, particularly the Merz Grade 4 jawlines (6) with extensive jowling. It has been the author’s experience the Merz grade 4 patients should be referred for a surgical consultation because nonsurgical measures are not usually effective. It must also be noted that younger females with wide lower faces will become wider with the enhancement reJAWvenation and that might not be a desirable feature. These patients will often require RF tightening and/or fat reduction to better define the jawline.
Enhancement reJAWvenation (7)
These patients have no obvious aging of the jawline and desire a more defined and attractive jawline. The goal is to highlight the border of the jawline and ascending ramus. Subtle chin augmentation is often performed as well. Blunt cannulas are the preferred method for the filler injection. Cannulas enable the injector to use one or two access points per side, minimizing tissue trauma and patient discomfort. The preferred entry point is at the area of the “future jowl”, anterior to the antegonial notch, along the inferior border of the mandible. The pilot hole is created just through the dermis. A cannula of 50mm, either 25g, 23g, or 22g is used and inserted into the subcutaneous, supraplatysma plane and directly posteriorly along the inferior border of the mandible. Stretching the skin overlying the mandible and parotid facilitates the advancement of the cannula. Once at the gonial angle and confirmed with the noninjecting hand, filler is injected in a retrograde fashion. Repeated passes are performed until the desired enhancement. Filler is also injected overlying the gonial angle in a radius of ~1.5-2 cms. To enhance anterior, the same entry point is used, and the cannula is flipped 180 degrees. With the noninjecting hand, the prejowl and chin area is lifted, and the cannula is punctured through the SMAS (platysma) and into the supraperiosteal plane. The cannula is advanced to the midline chin and then retrograde injection is performed. While not required for enhancement reJAWvenation, the injection should be between the mandibular osseocutaneous ligament and the platysma mandibular ligament. If further enhancement is desired, a second entry point is created at the gonial angle. The cannula is inserted in the subcutaneous plane and advanced along the posterior border of the ascending ramus. Retrograde injection is performed with mindfulness on the appropriate gender specific angles previously discussed. Further enhancement of the radius around the gonial angle can be accomplished if needed.
Restoration reJAWvenation (8)

These patients have jowling and notable aging along the jawline, chin, and prejowl sulcus. The entry point is now chosen as the lowest point of the jowls. This level becomes the new inferior border of the jawline and correction is made anterior and posterior to this point. A subcutaneous plane is used but the goal is to place below the inferior border of the mandible. (It is essential to avoid any deposition of filler in the jowl area.) Continue posterior to the area inferior to the gonial angle. The goal is to create a “neo-gonial angle” with the filler. The retrograde injection is performed in a “tadpole” fashion, with a larger deposition of the filler posteriorly and gradual less placement as the cannula moves anteriorly. The following pass is done in a separate tunnel that is inferior to the previous one with similar technique. This same process continues until the level of the inferior border of the mandible is aligned with the inferior aspect of the jowl. The cannula is flipped and turned anteriorly. The plane is switched to a supraperiosteal plane, between the mandibular osseocutaneous ligament and the platysma mandibular ligament. Injection is placed in this plane in the prejowl sulcus and chin if required. A more superficial plane for the marionette area is often required using the same entry point or through an entry just lateral to the marionette. Subcision of the labiomental ligament (a ligament originating from the DAO and inserting into the skin) is an essential compliment to the correction. (9) At the discretion of the injector, an enhancement of the posterior mandible is performed through a new entry point at the gonial angle and in a radius of ~ 1.5-2cm. Care must be taken to avoid too much filler in this area and exacerbating an already “heavy” or wide lower face.
The restoration reJAWvenation can often require 6-8cc of filler for optimal results. It is recommended that the procedure be divided into 2-3 sessions separated by 2-3 weeks if more than 6cc are required. If there is a significant fat component of the lateral jaw and upper neck, the procedure should not be performed and more invasive techniques should be considered, such as liposuction or surgery.
In a retrospective study, the author found that patients who were treated with multiple sessions and with higher volumes of filler had better clinical results (per Merz Jawline Scale) and were more satisfied with their treatments (GAIS Scale).



Filler choice
In general, fillers used for the reJAWvenation need to have a high G prime. The choice of filler is dependent on many factors – skin thickness, reversibility, patient wishes, and expected duration. If the patient’s skin integrity is poor and thin, the filler chosen must be forgiving, and a lower G prime hyaluronic acid filler is appropriate. For thicker skin, a high G prime HA filler, Calcium Hydroxylapatite, or PMMA can be used. Fillers that the author considers poor candidates are PLLA due to its low G prime and high diffusion and autologous fat which leads to poor definition of the mandibular border.
Importance of Plane of Injection
There are many injectors that use a needle technique onto the periosteum for the jawline. The author feels that while this is a viable option for the enhancement reJAWvenation, it has several drawbacks. By injecting onto the periosteum, there will be periosteal and masseter irritation leading to more post procedure soreness and trismus. In the area of the ascending ramus, parotid injection is possible with subsequent parotiditis as a result. Most importantly, is the possibility of intravascular in the facial artery which lies along the periosteum. Vascular occlusion can be completely avoided if the supraplatysma plane is used as describe with the author’s technique.
Injections that are placed more superficially tend to lead to more noticeable corrections than when placed deeply. In essence, the subcutaneous plane of filler will give “more bang for the buck” then supraperiosteal injections.
Placement of filler along the lateral aspect of the mandibular body will always lead to widening of the jaw and bigonial width. This is not desirable in the patient that require the restoration reJAWvenation because these patients are already “heavy” in the lower face. The supraperiosteal injections will actually be counterproductive in the older patients. Even if these injections were place on the inferior border of the mandible, the extent of mandibular body height improvement doesn’t compare to the author’s technique of filler placement in progressively lower tunnels under the mandible.
Neuromodulators
The platysma is broad muscle that arises from the upper chest and shoulder and extends superiorly above the mandible into the lower face. It is contiguous with the SMAS of the face. Upon contraction, it creates a negative vector on the lower face soft tissue, exacerbating the signs of the aging jaw. Relaxing the platysma with neuromodulation will result in a diminution of the negative/inferior vector leading to a net positive/superior vector on the jawline. The clinical outcome with be improvement in the jowling and a more defined mandibular boarder.
There are a few techniques described in the literature to inject the platysma. The most popularized method is called “The Nefertiti Lift” originally described by Dr. Phillip Levy in 2008. The procedure involves injections along the jawline and upper lateral platysma bands with a maximum of 20 onabotulinum toxin A. Another technique described by Woffles Wu in 2015 is “MicroBotox” and involves 100-120 injections of a 1cc solution of onabotulinum toxin (2.5cc saline/vial reconstitution) with 20-28units, 1cc per side. The injections are placed into the dermis in the lower face and neck. Studies comparing the Nefertiti vs the Microbotox showed the improvement in the jawline and jowl were better with the Microbotox and the Nefertiti achieve better results on the platysma bands. (10) A third technique involves injection in the most prominent platysma bands by pinching the bands followed by direct injections. The author’s clinical experience has shown the last technique provides the best results for the platysma bands in the appropriate candidate.
Deoxycholic Acid
Deoxycholic acid is a bile salt that is produced by the liver to aid in fat digestion. When injected, it will permanently destroy unwanted fat. Its FDA approval is for submental fat but recent usage has included the jowl and upper neck fat. The injections must be placed in the subcutaneous fat and remain superficial to the platysma. The primary risk of the off-label injections in injury to the marginal mandibular nerve. Small doses and lifting the jowl during injection can limit the risk. Nerve injury is always reversible and can last up to 6 weeks. Other side effects are swelling – up to 3 weeks, skin necrosis, and rarely, vascular occlusion. Multiple treatments are typically required. Recent use of cannulas for injection might allow for a more precise placement in the subcutaneous/superficial fat pads and is the author’s preferred method.
Radiofrequency
There are many RF devices available to create tissue tightening. The only effective treatments are when the temperature exceeds 65C, which is necessary for neocollagenesis and elastogenesis. Non penetrating RF devices are unable to achieve this temperature because the skin surface must not exceed 45C, and there is no way to obtain that much differential in temperature between the skin surface and deeper dermis. If the skin surface exceeds 45C, burns and PIH are likely. There are 3 ways to achieve >65C – RF microneedling, or subdermal heating using RFAL (RF Assisted Lipolysis) or RF cannulas. Fat remodeling is achievable with RF. RFM maximum coagulation depths are 3.5-4mm, but purposeful heating of fat with destruction is achievable in the jawline, submentum, and jowl area. More aggressive fat removal can be achieved with the subdermal applications of RF.
Lasers
To achieve skin tightening, nonablative and ablative laser can be used. Ablative laser will give more results, but have longer downtimes, more wound care, and higher risks of scarring, PIH, and hypopigmentation versus the nonablative lasers. The neck is particularly risky for ablative lasers and this is thought to be secondary to lower levels of sebaceous glands in the neck. While fractional lasers are safer than totally ablative lasers, they don’t achieve the same tightening the full field lasers produce. It’s the author’s opinion that the jawline and neck should be treated with RF over lasers when tightening is desirable.
Threads
There are 2 basic types of threads, smooth and barbed. Smooth threads are used to stimulate collagen and can be used in cases of enhancement reJAWvenation. The barb threads are able to lift, albeit to a minimal extent, the jowl and upper neck. While this technique is becoming quite popular, it’s the author’s opinion that the effect on the jawline and duration of results (6-9 months) doesn’t warrant the cost and potential for side effects (visible threads, puckering, infection, extrusion).
Summary
Improving the aesthetics of the jawline is an extremely popular procedure and is one of the most important areas of female/male attractiveness. Using the reJAWvenation techniques outlined in this article, significant changes can be achieved with little to no downtime or risk. Choosing the appropriate candidates and explaining achievable expectations is the key to patient satisfaction. Fillers can produce immediate visible results which is highly desirable amongst most aesthetic patients. Further refinements can be achieved using combination therapies, including RFM, which is particular good at tightening the upper neck and jawline.
References
- https://www.cell.com/trends/cognitive-sciences/comments/S1364-6613(99)01403-5
- https://www.insider.com/more-masculine-face-shape-more-likely-to-cheat-2019-4
- https://plasticsurgerykey.com/genioplasty/
- https://www.sciencedirect.com/science/article/abs/pii/S1010518215004278
- https://www.qoves.com/female-facial-attractiveness-what-is-the-ideal-female-jaw/
- https://plasticsurgerykey.com/standard-evaluation-of-the-patient-the-merz-scale/
- https://www.youtube.com/watch?v=3HVd0W2jZSI
- https://www.youtube.com/watch?v=Zpu-x-fZoJw
- https://nextstepsinderm.com/derm-topics/the-happy-face-treatment
- https://www.medestheticsmag.com/microbotox-versus-nefertiti-lift-lower-face-rejuvenation